Be forewarned, this is NOT another typical article on the importance of washing your hands and not touching your face, with the looming danger of the coronavirus.
As an avid researcher and geek in genetics, microbiology, and Environmental Medicine, I am super curious about this “new virus” and what solutions and problems lie ahead
I prefer to dive deep into the both the seen and the unseen, as well as the known and the unknown
There are many unknowns
As I observe this pandemic of confusion and fear, it reminds me of the famous (and very confusing) statement of the politically slippery Donald Rumsfeld in regard to the looming ‘weapons of mass destruction’…..stating that “there are many known-unknowns, and unknown-unknowns”
- Ok….so what do we actually know about COVID-19?
- Why is it spreading so quickly and not acting as the previous 2003 coronavirus?
- How does the genetics of COVID-19 interact with our genetics?
- Where did it come from and are certain people more susceptible?
- Since humans have co-evolved with viruses for time immeasurable, what is the big deal and why can’t we just support our innate immune response and go on with our lives?

Here is what we do know
One very important fact to keep in mind, is that this is a new virus. Everyone of us is susceptible, since our species has never met this invisible contagion or had the opportunity to build immunity.
Since we have not evolved with this particular virus, we can only learn as move through this together. I am beyond grateful to the providers and scientists who are working tirelessly, to crack the code of our new strain of coronavirus.
Now, let’s explore what has been ‘seen’ with this pandemic, such as the viral life span, level of contagion, and symptoms of infection.
According to Shenzhen Hospital (Guangdong Province, China) here is the most recent update on important findings:
THE SYMPTOMS
- It will first infect the throat, so you’ll have a sore throat lasting 3 / 4 days
- The virus then blends into a nasal fluid that enters the trachea and then the lungs, causing pneumonia. This takes about 5 / 6 days further.
- With the pneumonia comes high fever and difficulty in breathing.
- If you have a runny nose and sputum, you have a common cold
- Coronavirus pneumonia is a dry cough with no runny nose.
- This new virus is not heat-resistant and will be killed by a temperature of just 80 degrees F (It appears to hate the Sun).
Contagion and Prevention:
- If someone sneezes with it, it takes about 10 feet before it drops to the ground and is no longer airborne.
- If it drops on a metal surface it will live for at least 12 hours – so if you come into contact with any metal surface – wash your hands as soon as you can with a bacterial soap.
- On fabric it can survive for 6-12 hours. normal laundry detergent will kill it.
- Drink water. When droplets enter the mouth, they can be flushed in the stomach and destroyed by stomach acid. If they sit in the mouth, it will enter the sinuses and lung.
- Drinking warm water is effective for all viruses. Try not to drink liquids with ice.
- You should also gargle as a prevention. A simple solution of salt in warm water will suffice.
- Wash your hands frequently as the virus can only live on your hands for 5-10 minutes, but – a lot can happen during that time – you can rub your eyes, pick your nose unwittingly and so on.
Now for the more interesting ‘unseen’ part of the virus
The COVID-19 (coronavirus 2019) is also known as the SARS-CoV-2, meaning that it is a Sudden Acute Respiratory Syndrome derived from Coronavirus.
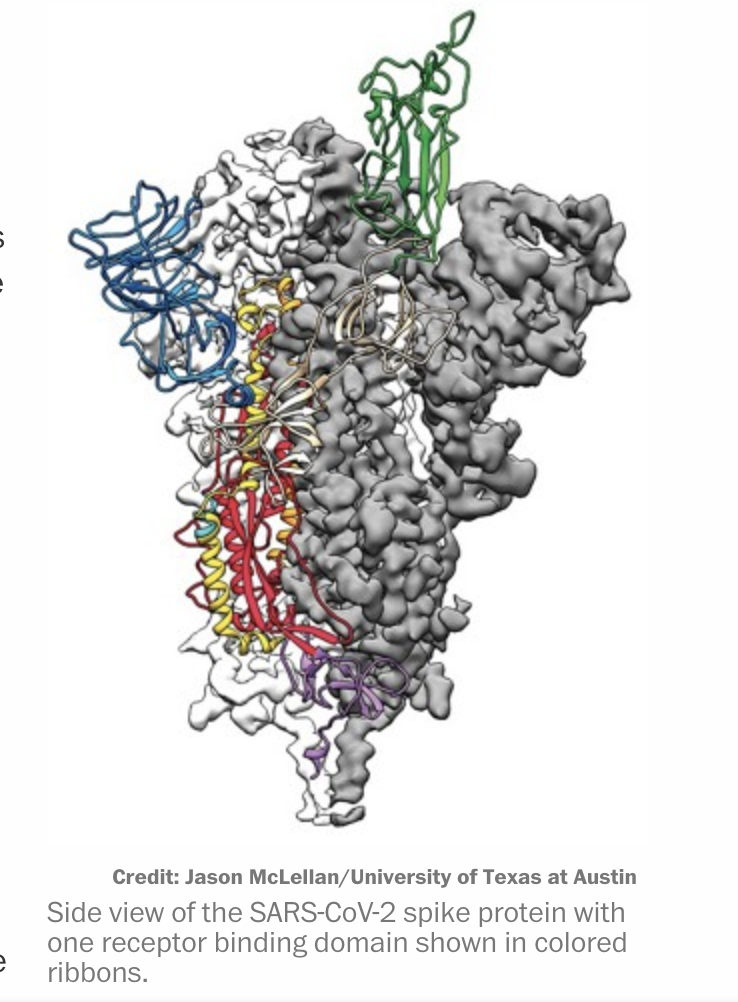
Just like the SARS virus (CoV-1) of 2003 and the Middle East respiratory syndrome (MERS-2012) viruses, this SARS-CoV-2 contains a spike protein that helps the virus attach and infect the human cell. (1)
Coronaviruses, in their chemical structure, are RNA viruses that typically enter human cells when their glycoproteins bind proteins on the cell surface.
The difference with this novel (aka new) virus, SARS-CoV-2 has an even stronger affinity for the ACE2 genetic enzyme than did it’s predecessor, SARS-CoV-1
“SARS-CoV-2 binds to the angiotensin-converting enzyme 2 (ACE2) on human cells with higher affinity than does the virus that caused severe acute respiratory syndrome (SARS) in 2003. This difference in affinity possibly explains why the novel coronavirus is more contagious than that other virus”. (1)
This is where it gets interesting….
You may not have heard of ACE2 (angiotensin-converting enzyme 2), found in human epithelial tissue, but you probably have heard of ACE2 Inhibitor drugs for blood pressure… more on this later.
There are ACE2 receptors in the epithelial tissue of the heart, kidney, the intestines, and in the lung.
The SARS-CoV-2 enters the lung through droplets and the receptor for the virus is the ACE2 in the lung.
“Human ACE2 appears necessary and sufficient to serve as a receptor for SARS-CoV” (2)
This leads me to three questions
- Will those of us with ACE2 polymorphism be more vulnerable to the infection?
- Does the solution to this infection lie within the ACE2 enzyme activity?
- What are the other genetic enzymes involved?
As you know, one gene never works in isolation, plus the more we learn, the more we need to learn…
First lets look at ACE…

What does Angiotensin-converting enzyme do?
The ACE2 enzyme (rs2106809) has been studied for its role on regulating blood pressure.
Angiotensin-converting enzyme (ACE) is actually central in the RAS (renin-angiotensin system), which regulates blood pressure by regulating the volume of fluids in the body.
It does this my converting the hormone angiotensin-l into the active vasoconstrictor angiotensin-ll
Both ACE2 (rs2106809) and ACE1 (rs4343) have receptors throughout the epithelial tissue in the body
With ACE2 in the lungs acting as the SARS-CoV receptor, this virus can then access the control panel for fluid in the lungs and vasoconstriction of fluid and air in the lung.
An interesting position for an outside virus to access
How does ACE2 impact COVID-19 infection?
As mentioned before, scientists have shown that the ACE2 is the receptor for SARS-CoV-2 (aka COVID-19)
The ACE2 gene encodes the angiotensin-converting enzyme-2, which has been proved to be the receptor for both the SARS-coronavirus (SARS-CoV) and the human respiratory coronavirus NL63, and is the proven host receptor for the novel coronavirus 2019-nCoV/SARS-CoV-2 (4)
Previous studies demonstrated the positive correlation of ACE2 expression and the impact of the SARS-CoV infection, (in vitro).
Studies also showed that the number of ACE2 variants (type of mutation) could reduce the association between ACE2 and S-protein in SARS-CoV or NL63.
Therefore, the expression level and expression pattern of human ACE2 in different tissues might be critical for the susceptibility, symptoms, and outcome of 2019-nCoV/SARS-CoV-2 infection. (4)

ACE2: More prevalent in Asia?
It is not clear how certain regions and populations share common genetic mutations.
Whether this is part of the human genetic relationship with the genetics of local viruses and bacteria, or that certain regions have particular toxic exposures (such as pollution in air and water, or shifts in the microbiota), we do know that statistically the Chinese have a higher prevalence of certain genetic polymorphisms, including ACE2 and MTHFR.
The East Asian populations have much higher AFs (allele frequency) in the eQTL(expression quantitative trait loci) variants associated with higher ACE2 expression in tissues, which may suggest different susceptibility or response to 2019-nCoV/SARS-CoV-2 from different populations under the similar conditions.(4)
This may explain one reason why these SARS outbreaks start in China (the other possible reasons, I will mention later).
ACE2 mutation + COVID-19 = Fatalities?
A recent single-cell RNA-sequencing (RNA-seq) analysis indicated that Asian males may have higher expression of ACE2 (7)
Looking at the data of infection and fatalities from COVID-19, it has impacted more Asian males than females.
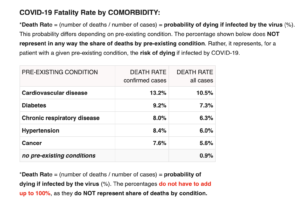
Even more interesting, is when the data of fatalities in association with pre-existing conditions, cardiovascular disease surpassed all other possible conditions, as mentioned before, ACE2 is involved in cardiovascular disease
Now this is where I would like to introduce another gene enzyme which is involved in glucose and immune regulation.
Dipeptidyl peptidase-4 (DPP4), also known as adenosine deaminase complexing protein 2 or CD26, is the genetic enzyme closely associated with diabetes and various cancers. *(If you look at the graph above, diabetes is second on the list).
DPP4 is also of interest in this pandemic, with its unique relationship with MERS.

The Plot Thickens
Is it just me, or do these genes look like incredible pieces of art…. but I do digress. As mentioned before, there is never just one gene (or one microbe) that is solely involved in disease and infection.
Our microbiota (the community of trillions microbes in and on our body) works like an intricate ecosystem to support our human genetic blueprint. After all, we are simply a walking and breathing host for an invisible life force of microbes that is dedicated to keeping us healthy and alive.
Science has confirmed that CD26/DPPIV plays an important role in tumor biology, diabetes, and also as a receptor site for coronavirus.
Middle East respiratory syndrome-related coronavirus (MERS) has been found to bind to DPP4. It is found on the surface of cells in the airways (such as the lungs) and kidneys. Scientists may be able to use this to their advantage by blocking the virus’s entry into the cell. (12)
Interestingly, serum sDPP4 activity can be associated with the progress of COPD (chronic obstructive pulmonary disease), meaning high correlation with respiratory inflammation.
DPP4 is found on the surface of cells in the lung and airways, and in the kidneys. Researchers are using this to an advantage as a way to block viral entry into the cell.
A class of oral hypoglycemics called Dipeptidyl peptidase-4 inhibitorsworks by inhibiting the action of this enzyme, thereby prolonging incretin effect in vivo.(11)
Please know, that I am not suggesting genetic manipulation to combat these new viruses, I am simply exploring how our unique genetic blueprint plays a role in susceptibility.

Exposure vs. Impact
Clearly there is massive fear on exposure to the COVID-19, but exposure does not quantify or qualify the impact on the individual.
This is where I would like to interject some positive news.
We know that this highly contagious virus is moving like a tsunami throughout the world, causing terrible casualties…however, there are more people who survived and recovered, than those who have parted. (Presently 5,821 parted and 74,460 recovered)
One woman in Washington state, has recovered from CoVID19 and reported symptoms similar to a flu. She was tested positive, but did not experience severe respiratory issues.(10). Her message on the news, was “try not to panic.”
People who are young with a strong immune system (gut health & genes), should take precautions but consider this as a horrible new flu. Please have compassion for the elderly and the health compromised. Practice respectful social distancing to remove the mass burden on the medical system and allow elders the resources needed.
A little story of mine…
Before I started to geek out on genetics, my fiancé and I traveled to Brazil on a flight connecting from Asia, in 2003.
I had no idea about SARS or why everyone on the plane was coughing, and why we were the only ones not wearing masks. *(Remember this is 2003, before social media)
Long story short, I contracted some sort of Acute Respiratory Syndrome, and it sucked! I would never wish this on anybody.

Miraculously, my fiancé escaped with nothing but concern for my condition.
I presented with a sore throat, fatigue, fever, and a spasmodic cough for days & nights, with no relief.
My uncle in northern Brazil, connected me with a doctor in Rio who treated me with medication through a nebulizer…brilliant treatment method, in retrospect and maybe something to be considered for acute treatment with CoVID-19.
Thankfully, because I was young & healthy, I recovered well and have not thought about it again…until now.
I did not have a confirmed positive test for SARS from coronavirus (once again…this was 2003), so I am not certain what I had, but if it was…do I have immunity?
Of course, immunity would be awesome, because not only do I not want to go through that again, but now I understand my unique predisposed, (although, this virus is not the same as the 2003 SARS).
How Are Treatments Influenced by Genetic Research?
Possible Treatments….the Known Unknowns…
We know that ACE2 plays a vital role in SARS, and DPP4 plays a role in MERS infection susceptible, but what to do with this information. (I will be interesting to see what pharmaceuticals will be trialed with this information).
This finding could greatly impact the development of effective SARS therapies. For instance, soluble forms of ACE-2 or anti-ACE-2 antibodies might be used to block SARS-CoV-binding to the receptor. Stimulated by potential roles in cardiac function and RAS, small molecule inhibitors of ACE-2 proteolytic activity have already been designed.
Future studies will likely reveal whether these compounds, or others more specifically intended to target the SARS-CoV binding site, will be effective in disrupting the interaction between virus and receptor.(5)
On another note, it appears the antivirals that worked on SARS in 2003, namely Remdesivir, which did not work on Ebola, are being presently tested on COVID-19. (3)
There has been positive results with Remdesivir with cases in both China and Washington state, so this may be what slows down the impact of this highly contagious form of SARS.

Supporting proper gene expression…
Since you cannot change your genetic blueprint, the only option is to support the expression of our genes.
This can be done through nutrients, although it is the microbiome (our microbial DNA) that is responsible for how the human genes express.
With Nutrigenomics (how nutrition influences gene expression), we have been able to relate certain nutrients with the up regulation or down regulation of a genetic enzyme, such as MTHFR and folate converting into methyl-folate.
We can see that ACE2 polymorphism is not influenced by a single nutrient, but by the broad umbrella of malnutrition and decreased ecology of the microbiota.
Of course, we may be able to pinpoint the important role of potassium or zinc with the ACE2, (since ACE is a zinc metalloendopeptidase), but the role of the microbiome on human gene expression is more complex than simply that.
(Ace2), which encodes a key regulatory enzyme of the renin-angiotensin system (RAS), results in highly increased susceptibility to intestinal inflammation induced by epithelial damage. The RAS is known to be involved in acute lung failure, cardiovascular functions, and SARS infections. Mechanistically, ACE2 has a RAS-independent function, regulating intestinal amino acid homeostasis, expression of antimicrobial peptides, and the ecology of the gut microbiome. (6)
So if the microbes determine human gene expression, and these impacts the health of the gut microbiota, shouldn’t we focus on this mechanism?

Your Microbes Hold the Key…
Over 90% of our immune response is dictated by our microbiota, throughout our digestive tract from mouth to colon.
Studies have correlated multiple disease states, including auto-immunity and systemic inflammation, with low diversity in the microbiota.
We have trillions of microbes that live in and on our bodies, forming an ecosystem that regulates and fends off external viral, bacterial, and fungal invaders.
It seems rational to conclude that feeding your microbes, (promoting microbial diversity), will support the innate immune system, providing the reserves to confront COVID-19.
Since I understand that I may be more susceptible, this is exactly my tactic. I am feeding my microbes with resistant starches, and taking high Bifido stains of probiotics, among other practices to support my overall health.
Support Your Blueprint:
Clearly the most important focus should be feeding your microbes, which are in charge of your immune system and gene expression.
Also nutrients and food that have shown to support genetic expression of ACE and DPP4 are the following: D-Mannose, L-Proline, Zinc, Holy Basil (Tulsi), White Mulberry, Guava, Jackfruit, Grapes, Apples, Onions, Green Tea, Black berries, Raspberries, Broccoli, Brussel sprouts, Cucumber, Potatoes, Tomatoes, Lettuce, Green beans, Rhubarb, plus many fermented prebiotic foods.
Because of my genetic blueprint, I am presently supplementing with Vitamin D3/K2, liposomal Vitamin C, Glutathione with methylated B-vitamins, resistant starch fiber, and the herbal formula Jade Wind Screen. *Very important to note this is not medical advice, and not meant to substitute advice from your primary healthcare practitioner.

How to Test Your Blueprint
This information will be available in other articles, since there is too much information to fit on this page.
However, I will mention that to test your microbial DNA (your microbiome) there are a couple home tests kits I recommend, namely BiomeFx by Microbiome Labs or Thyrve home kit by Thryve.
For human genetic testing, the standard is 23andme, although there has been more shifts and restrictions on available data over the last few years. AncestryDNA also provides home kits, but The main difference between 23andme and AncestryDNA is that 23andMe offers gene testing for health analysis, and AncestryDNA is much more focused on genealogical.
There is a new company called NutriGenetic Research Institute, that is providing more health data than any other company.
It is helpful to have analysis support through someone trained in Nutrigenomics.
There are multiple programs we use to plug in the raw data to retrieve the SNPs and CYPs that are embedded in the data, such as TrueReport and StrateGene.
However, for a simple analysis of your 23andme test, you can plug your raw data into GeneticGenie.org (the sister program to 23andme), to have a print out of your genetic profile.
Now here’s what we do not know
We do not truly know how or where this mess started, or how will it end. Although many of us in the field of Environmental Medicine saw it coming.

The Unknown Unknowns…
Where this virulent virus began is still one of the “unknown unknowns”
Was it the “wet market” in Wuhan or the National Biosafety Laboratory, at the Wuhan Institute of Virology?
Either place represents epic nightmares for me.
In the wet market there are thousands of caged animals, stacked upon each other, and slaughtered on site without any precaution for sanitation, or prevention for cross infection and exposure to other animals. (9)
Not only is this an inhumane treatment of animals, but very dangerous for exposure to coronaviruses that are common in many animals, especially bats. *(At the time of writing this, the Chinese government is threatening to make all wet markets illegal)
As for the lab, it is overwhelming to imagine what is going on behind closed doors in the world of bio-engineering.
China is not the only one in the race to manipulate microbes…universities and corporations within the US have also been genetically modifying viruses, bacteria and funguses, in the name of research and medicine.
The US has also been genetically modifying food for decades, and we are still unclear how these modifications are impacting our own genetics or biochemistry.
We can only speculate where this coronavirus mutated and gained it’s super power.
Believe me, I am lover of the X-files and Stranger Things, as much as anyone else, however I am leaning towards an unfortunate cross infection from improper treatment of animals.
Whichever, the virus is now with us, and we need to deal with it.
In the wise words of an African proverb:
If the snake is in the tent, first deal with the snake before you look for the hole in the tent, where the snake entered.
The Bigger Picture
Clearly, we do need to deal with this pandemic (the snake), but also look at the bigger picture of how we created a tent with so many holes in it.
It is essential to focus on prevention of further outbreaks, with even deadlier viruses, and this can be done by focusing accountability on corporations and reversing the ‘learned helplessness’ of the masses who are oppressed by governments that lack foresight, or think that climate change is a hoax.
In other words, if we look at the big picture, we have reached a tipping point where we have over burdened the Earth with pollution and toxic chemicals, to feed our endless demand for objects we do not need.

China has become the world’s factory, with the highest concentration of pollution, and not surprisingly has the largest population of certain genetic mutations, such as MTHFR and ACE2.
This endless burden on China, will create greater fallout of epidemics that will sweep throughout the world.
None of us are immune to the mess we are creating
I hate to say this, but there is a poetic justice that this invisible grim reaper has been named corona….which means the female crown. Mother Earth has taken back the thrown, and the wrath of our abuse is coming back to haunt us. It truly doesn’t matter if you are an ecological warrior, we won’t be differentiated, for she can no longer tolerate the cancerous growth of the overdeveloped human race.
Where to go from here?
Of course, I don’t want to leave you deflated and without hope.
Please heed the advice of keeping yourself healthy with this pandemic.
My simple advice is to feed your microbiota, which will both support your immune system and regulate your gene expression.
If you are interested, I am offering the first educational video of my 6 part course on Feeding Your Microbiome as a free gift

As we focus on resolving this pandemic and preventing further deadlier pandemics, we need to commit to reducing the body burden on both the planet and your physical body.
The connection of our internal ecology with the external ecology was the basis of all ancestral medicine (ie. Ayurveda and Classical Chinese medicine), but somewhere along the way our health philosophy and practice devolved into a separation that has had dire consequences.
It is time to wake up to the fact that climate change is happening, both around us and inside us
Resources:
- Structure of novel coronavirus spike protein solved in just weeks https://cen.acs.org/analytical-chemistry/structural-biology/Structure-novel-coronavirus-spike-protein/98/i8
- ACE2 Receptor Expression and Severe Acute Respiratory Syndrome Coronavirus Infection Depend on Differentiation of Human Airway Epithelia https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1287568/
- Remdesivir https://en.wikipedia.org/wiki/Remdesivir
- Comparative genetic analysis of the novel coronavirus (2019-nCoV/SARS-CoV-2) receptor ACE2 in different populations https://www.nature.com/articles/s41421-020-0147-1
- ACE-2: The SARS Receptor Identified: https://www.rndsystems.com/resources/articles/ace-2-sars-receptor-identified
- ACE2 links amino acid malnutrition to microbial ecology and intestinal inflammation: https://www.nature.com/articles/nature11228
- Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCov https://www.biorxiv.org/content/10.1101/2020.01.26.919985v1
- Both the new coronavirus and SARS outbreaks likely started in Chinese wet markets: https://www.businessinsider.com/wuhan-coronavirus-chinese-wet-market-photos-2020-1
- Coronavirus: Injected US woman talks about her symptoms and recovery from Covid-19: https://www.independent.co.uk/news/world/americas/coronavirus-symptoms-recovery-time-immune-covid-19-washington-seattle-a9400331.html
- Dipeptidyl peptidase-4: https://en.wikipedia.org/wiki/Dipeptidyl_peptidase-4#cite_note-pmid23486063-19
- Adaptive Evolution of MERS-CoV to Species variation in DPP4: https://www.cell.com/cell-reports/pdf/S2211-1247(18)31148-3.pdf
 Read Previous Post
Read Previous Post
